


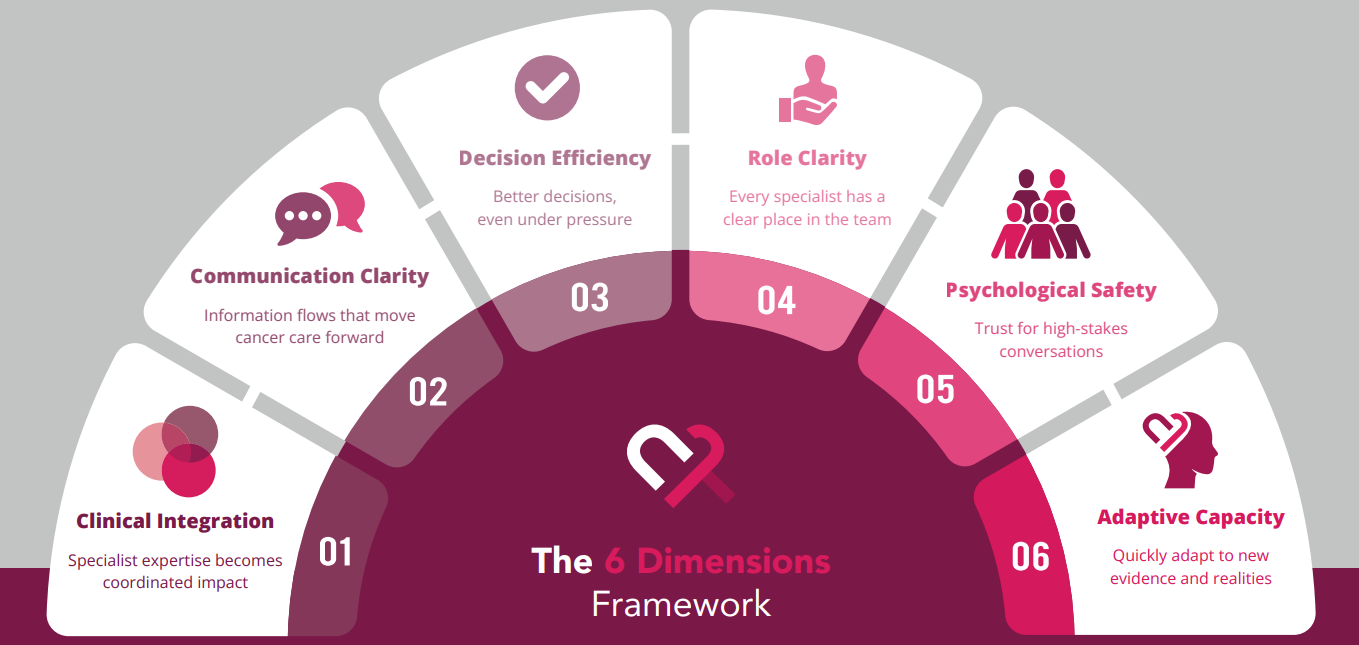
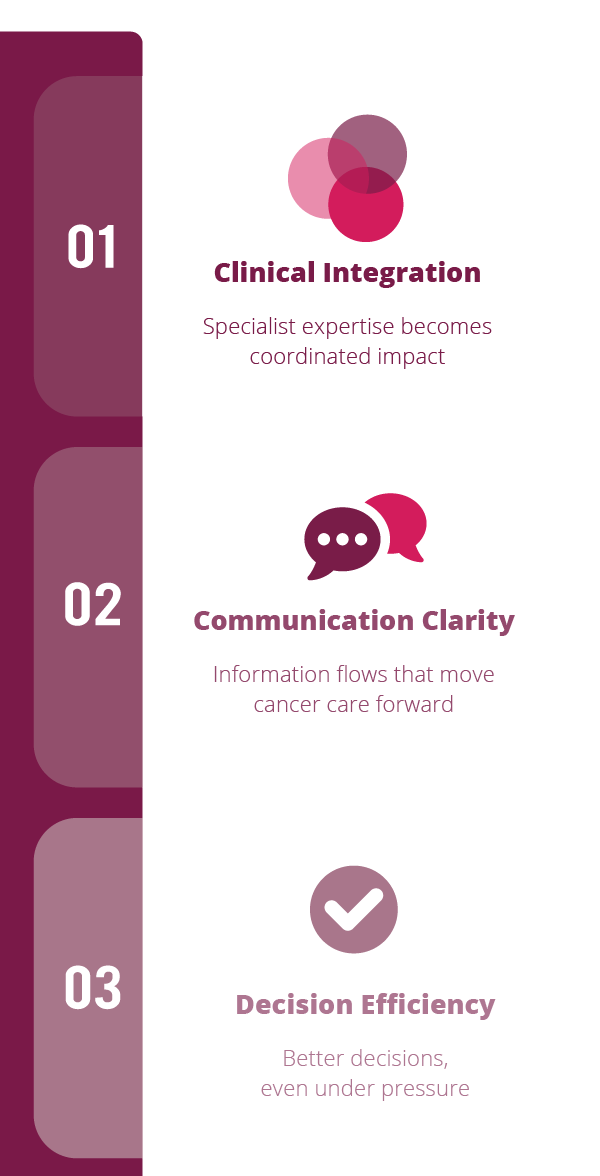

1. Clinical Integration
 Specialist expertise becomes coordinated impact
Specialist expertise becomes coordinated impact
Systematic specialist coordination explains 52% of variance in treatment decision quality across 822 cancer case discussions in multidisciplinary team meetings (Soukup et al., 2020)
A HER2-positive, metastatic breast cancer patient, second progression with brain metastases. This case is on the tumour board agenda next Tuesday.
Before the meeting opens, who needs to have said what, to whom?
When it holds:
- One plan leaves the room
- Handovers carry the clinical nuance, not just the decision
- Specialists feel their expertise was used, not just noted
When it breaks:
- Critical input arrives after the plan is set
- The same case gets re-discussed because something was missing
- Parallel thinking, not integrated thinking
The instinct when integration breaks is to say the team needs to communicate more. The research shows the opposite. During coordination failures, information quality drops as communication volume rises.
Coordination in cancer care is assumed, not built. It is supposed to happen. When it does not, the automatic read is individual failure. The structural read is that nobody designed how the integration should work before the meeting began.
What do you see from where you are?
2. Communication Clarity
 Information flows that move cancer care forward
Information flows that move cancer care forward
Structured tools improved MDT decision-making from 82% to 93%, with clinicians reporting smoother teamwork (Brown et al., 2022).
Colorectal liver metastasis recurrence. The case was discussed at the last tumour board, a plan was agreed. A week later, it turns out the oncologist and the radiologist had been referencing different scans mid-discussion.
When your team leaves a case discussion, how do you know you left with the same picture?
When it holds:
- The right information reaches the right person at the right time
- People leave conversations with the same picture
- What was said matches what was heard
When it breaks:
- The room moves forward on information that was never actually shared
- Handovers carry the decision but not the nuance
- Misunderstanding surfaces only when something downstream goes wrong
The instinct when communication breaks is to add more structure. Protocols, templates, checklists. The research points the other way: structured tools reduce errors in urgent handoffs, and the same rigidity makes complex case communication worse. Staff who adapt style to context are not failing protocol. They are using judgement.
Communication quality is not measured by what was said. It is measured by whether what was said was registered, and matches what was received. Confident disclarity is what happens when a team leaves a conversation convinced it reached shared understanding, and only discovers later that it did not.
What do you see from where you are?
3. Decision Efficiency
 Better decisions, even under pressure
Better decisions, even under pressure
Decision quality drops after 20 cases — but short breaks fully reverse this decline (Soukup et al., 2019).
A rare ovarian sarcoma opens the tumour board meeting. The room is fresh, the discussion is deep, the focus is real, the decision takes the time it needs.
Two hours in, an abdominal soft tissue sarcoma is discussed briefly. Seen before, straightforward, decided in three minutes.
What if these were discussed in the opposite sequence? Which case gets the more optimal decision?
When it holds:
- Timely decisions reached with the right input
- Clear ownership of what was decided and who implements
- Cognitive quality holds across the whole agenda, not just the opening cases
When it breaks:
- Decisions drag or get revisited at the next meeting
- Late-agenda cases feel efficient in the moment and thin on review
- Fatigue gets attributed to complexity or personality, never to the structure
The instinct when decisions feel slow is to tighten the agenda, move faster, push through. The research points the other way. Decision quality holds through the first ten to twenty cases, then drops. A short break and a clear summary at the point of decision recover what speed alone cannot.
Fatigue and familiarity together produce decisions that feel clear and are not. The late-agenda case gets one or two minutes and feels efficient. The gap only becomes visible when the plan turns out to have missed something, or when nobody quite remembers what the plan was.
What do you see from where you are?
4. Role Clarity
 Well-defined roles, invisible work made visible
Well-defined roles, invisible work made visible
Role clarity is systematically underdeveloped in MDTs, limiting execution even when discussions are strong (Horlait et al., 2019).
Think of the person on your team who quietly carries the coordination. Who chases the referral when nobody else does. Who keeps track of which scan is missing, which consent is pending, which follow-up has not been booked.
What is their formal role? What work do they actually do?
When it holds:
- The work that keeps the team running is visible to the people who staff it
- The person doing coordination is the person recognised for it
- When they are on leave, the team feels it structurally, not personally
When it breaks:
- The team runs because one or two people carry the invisible load
- They are experienced enough to carry the work, not senior enough to be recognised for it
- The role on paper and the role in practice have quietly drifted apart
Coordination work is often done by people close enough to the patient to see what is needed, and not senior enough to be at the table when the work is named. It becomes invisible by becoming reliable. When the work is absorbed without friction, the system stops seeing it.
The role clarity problem is not usually that people do not know who does what. It is that the ones doing the most are the ones least recognised for doing it. The team finds out what was holding it together when the person holding it leaves.
What do you see from where you are?
5. Psychological Safety
 A space built by the team, not a trait of the people in it
A space built by the team, not a trait of the people in it
71% of European young oncologists report signs of burnout, with regional rates as high as 84% (Banerjee et al., 2017).
A junior colleague sees something in a case that does not fit the plan. Not a critical error. A question worth asking. The room is senior, the discussion is moving, the decision is near.
Do they speak? And what in the room — not in them — decides the answer?
When it holds:
- The question gets asked, and the team is better for it
- Disagreement surfaces in the room, not in the corridor afterwards
- Mistakes get named early enough to course correct
When it breaks:
- The concern arrives after the decision, through a side channel
- People learn, without being told, what is safe to say and what is not
- The team hears agreement and assumes alignment
The instinct when burnout rises is to offer wellness programmes. The structural read is that burnout and silence often share a cause. Psychological safety is a property of the team, not of the individuals in it. The same hospital can hold teams where voice flows and teams where it does not, sitting in the same building, under the same hierarchy, with the same pressures.
What differs is who speaks first, how questions are received, and whether the leader treats uncertainty as risk or as information. Whether a junior colleague speaks up in a hard moment is decided long before the moment arrives, by what the team has learned about what happens to people who do. The leader's sphere of influence here is larger than most leaders assume.
What do you see from where you are?
6. Adaptive Capacity
 Coordination that holds when the context changes
Coordination that holds when the context changes
Teams with strong adaptive processes implement evidence-based practices 3–5 times faster (Nilsen & Bernhardsson, 2019).
A new AI triage tool goes live on the team's workflow this quarter. It is well-validated. The vendor has run the training session. The consultant champion is enthusiastic.
Who on the team knows how it changes handovers? Who decides what it means for the nurse's role, the coordinator's role, the junior's role?
When it holds:
- New tools and new evidence get absorbed into how the team actually works
- The team adapts together, not each person on their own
- What the team learns from using something new feeds back into how it uses the next thing
When it breaks:
- The tool is live, and the team's practice around it forms by accident
- Some people integrate it, others work around it, and nobody has named the gap
- The next new thing arrives before the team has finished absorbing this one
AI amplifies what is already there. On a team with strong coordination, new tools extend capacity. On a team where coordination was assumed rather than built, new tools reveal the gap, usually by making it worse first.
Adaptive capacity is the difference between a team that is coordinating and a team that has coordinated. The first depends on the people present today. The second has turned what works into something the team owns — visible enough to induct someone into, durable enough to absorb what comes next.
What do you see from where you are?